
Physician innovators disrupt endoscopic visualization
Urology entrepreneurs Neal Patel, MD, and Philip Zhao, MD, proudly tout their handheld, wireless endoscopic camera as a device “designed by urologists for urologists."


Neal Patel, MD



Philip Zhao, MD

Their disruptive vision began one night during their urology residency. Waiting hours for staff to find a standard endos- copy video tower, future urology entrepreneurs Neal Patel, MD, and Philip Zhao, MD, wondered why such a bulky, inconvenient system had never been modernized.
Fast forward to today, where Patel and Zhao have turned their disruptive dream into a reality with the revolutionary Endoluxe system, a wire- less, high-definition (HD) endoscopic camera platform that replaces the antiquated towers.
Endoluxe is a handheld, portable orb containing an HD camera that can be attached to rigid or flexible analog endoscopes. This smart device captures images and video that are wirelessly streamed to any HDMI-enabled monitor display or cloud applications. Endoluxe also includes a software platform with cloud-based storage, as well as artificial intelligence (AI) /machine learning (ML) applications. According to the inventors, the AI/ML functionality “provides clinicians with anatomy recognition, structure identification, anatomic configuration, and suggested therapy.”
The Endoluxe system also provides urologists with a cost benefit, as it is available for a fraction of the cost of purchasing a tower. The device has been used by over 15 physicians on more than 1000 cases. Regarding regulatory status, Endoluxe received a class I exemption from the FDA in 2017, and the company anticipates filing this year for a breakthrough technology designation on AI/ ML for benign prostatic hyperplasia.
In a recent interview with Urology Times, Patel and Zhao discussed their personal journey and game-changing product, which they proudly tout as a device “designed by urologists for urologists."
Please provide some background on the development and use of your innovation.


The handheld Endoluxe system

Patel: What we as urologists and most endoscopists and surgeons use on an almost-daily basis is a camera looking inside some part of the body or an endoscope inside a part of the body, and the camera is attached to the endoscope, and you’ve got a light source attached to the endoscope to illuminate the cavity. And all these cords then come off your scope and attach to a very expensive, tall, bulky tower that sits in either your procedure room or the hospital. And through that, you’re able to visualize what you’re seeing on a screen and do what you need to do. And sometimes, if you don’t have any of that, you will put your eye up to the end of the scope and just look with 1 eye like they did 100 years ago. You will find many urologists in community clinics who are still doing that.
And the reason is, a lot of times these towers are very expensive. Starting prices are sometimes $20,000 to $30,000. That’s a huge fixed capital cost for a urologist, especially in the community. In the hospital, where sometimes their cost is less of a concern, some of these towers will cost upwards of $100,000 for all the visualization equipment that you need to do laparoscopic surgery, cystoscopy, and ureteroscopies.
And so, we came to the realization we can make this smaller and began work on designing the product that exists today, which basically takes that very large, 200- to 300-lb tower with a screen and all the cords coming off it attaching the scope, and we shrank it into something drastically smaller. Not only that, it’s a fraction of the cost of the tower.
What has been some of the feedback you have received from physicians using the device?
Zhao: One user said the first time he used Endoluxe, he felt like it was the first time he saw and felt an iPhone in his hand. It was something that was completely different from anything that he had ever used before—providing a complete degree of freedom without being tethered by any wires and not confined to any particular monitor. You can use any monitor with Endoluxe. You could go to Best Buy down the road and buy any monitor with HDMI input, and our system will wirelessly connect to it.
Please discuss the data/image storage and sharing functionality of Endoluxe.
Patel: We built all the data recording into our system. You can record with 1 touch. You can take a picture with 1 touch. It’s all very seamless to do and it’s all auto-syncing, all automated, and it goes into the cloud or the local electronic medical record system where it can be pulled up. We have a very robust web platform that you can log into, pull all your patient videos, and share with your patients and collab- orate with other physicians. It’s basically this giant digital platform for endoscopic media.


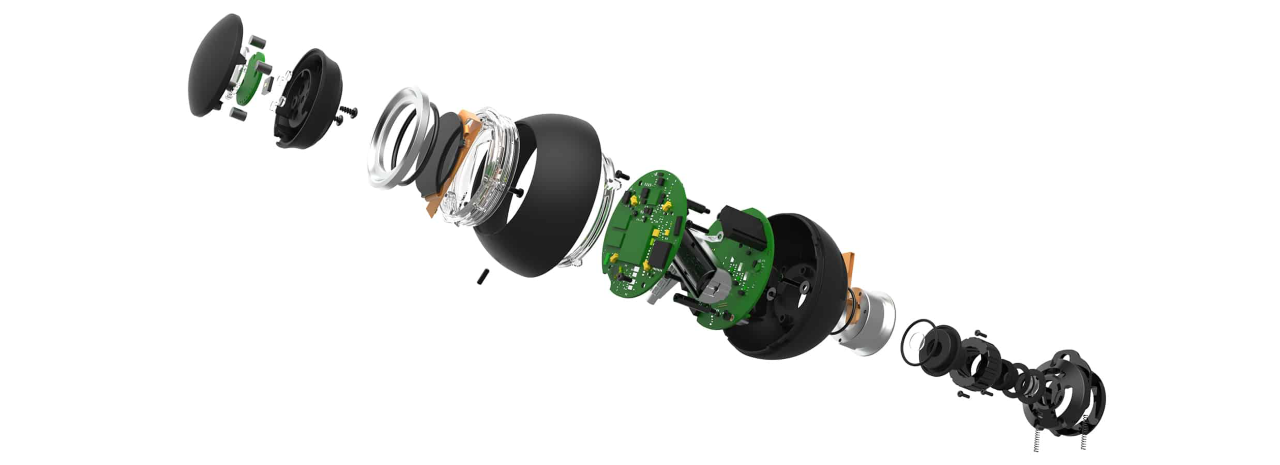
"Exploded" view of Endoluxe system
It’s been a great thing because we’re finding that patients are more adherent to their treatment plans if they actually can see what you see. In the past, we were not making these media recordings for various reasons, but I think now it’s going to become a mainstay. As a clinician, I’m seeing more and more requests every week for patients to see pictures of inside their body; they want to see how the treatment is helping, or how the tumor looks, or how the stone looks. And it just helps them understand what they need to do next and not be frustrated with their care and be more adherent. And so we built this digital health platform that goes along with our device that helps us to do this.
What has the Endoluxe experience meant to you?
Zhao: A lot of people in medicine have ideas about how to improve patient outcomes, increase clinical efficiency, and make surgeons’ lives easier. Because we’re all so busy, no one really takes the time to jump into a project and go the distance to build something great. We were willing to take that initiative.
Patel: We came up with the idea of this tech- nology many, many years ago. And as urologists in residency at the time, we had no idea how to create a device or get it to market or commercialized or really anything about a company. And so, we’ve had a very interesting and awesome journey, both as entrepreneurs and as clinicians.
In addition to cofounding Endoluxe, Patel is chief technology officer and director of Robotic Surgery at Advanced Urology, and Zhao is chief of the Urology Stone Program at Tisch Hospital, NYU Langone Health and an assistant professor of urology at NYU Grossman School of Medicine.











Investigators prepare for first-in-human bladder transplant study
September 13th 2023"Our study is the first report of bladder auto-transplantation in heart-beating, brain-dead human research donors as a necessary preparatory step toward clinical bladder transplantation in living patients," says Inderbir S. Gill, MD.


Dr. Benjamin N. Breyer appointed chair of the UCSF Department of Urology
August 24th 2023Benjamin N. Breyer, MD, is a urologic surgeon who is internationally known for performing complex urethral and penile reconstruction for urethra stricture and cosmetic disfigurement, male incontinence, male fistula, and surgery for erectile dysfunction.

Study set to explore the impact of peer-support for patients undergoing gender-affirming surgery
July 21st 2023"Extra support from trusted peers can help make navigating complex health care systems easier for transgender patients, who often have to wait years before receiving gender-affirming genital surgery—while also managing the stress and trauma associated with being part of a society that often doesn’t accept non-conforming gender expression,” says Geolani Dy, MD, FACS

